From DICOM to MPR (part 1)
This is the first part of 5 parts series. Link to part 2.
In this series of articles, we will review some obscure piece of technology that you probably never heard of but which may have saved your life at some point. We will cover a little of history, do some math and, most importantly, have fun !
Medical imaging is a pretty old field of science that was kick-started more than 120 years ago when Wilhelm Conrad Roentgen accidentally took the first radiography of his hand. He just discovered X-rays, a electromagnetic radiation which is sufficiently energetic to go through, with varying degree of efficiency, most of the human tissues. Although the term x-ray seems mysterious, there is nothing particular to them compared to other radiations with different energy levels. The spectrum of electromagnetic radiation also contains visible light, ultra-violet, infra red, gamma rays, radio waves or micro waves. The difference between those different "rays" or "waves" are just their frequency which is inversely proportional to their energy level. The more energetic a ray is, the more chance there is for the ray to be able to go through matter (which happens to be mostly empty space). Visible light for example is not able to go through your body, as Diogenes reminded Alexander the great, but x-rays can. In turn, x-rays can't go though thick sheets of lead for example, which is why this material is most often used for shielding.
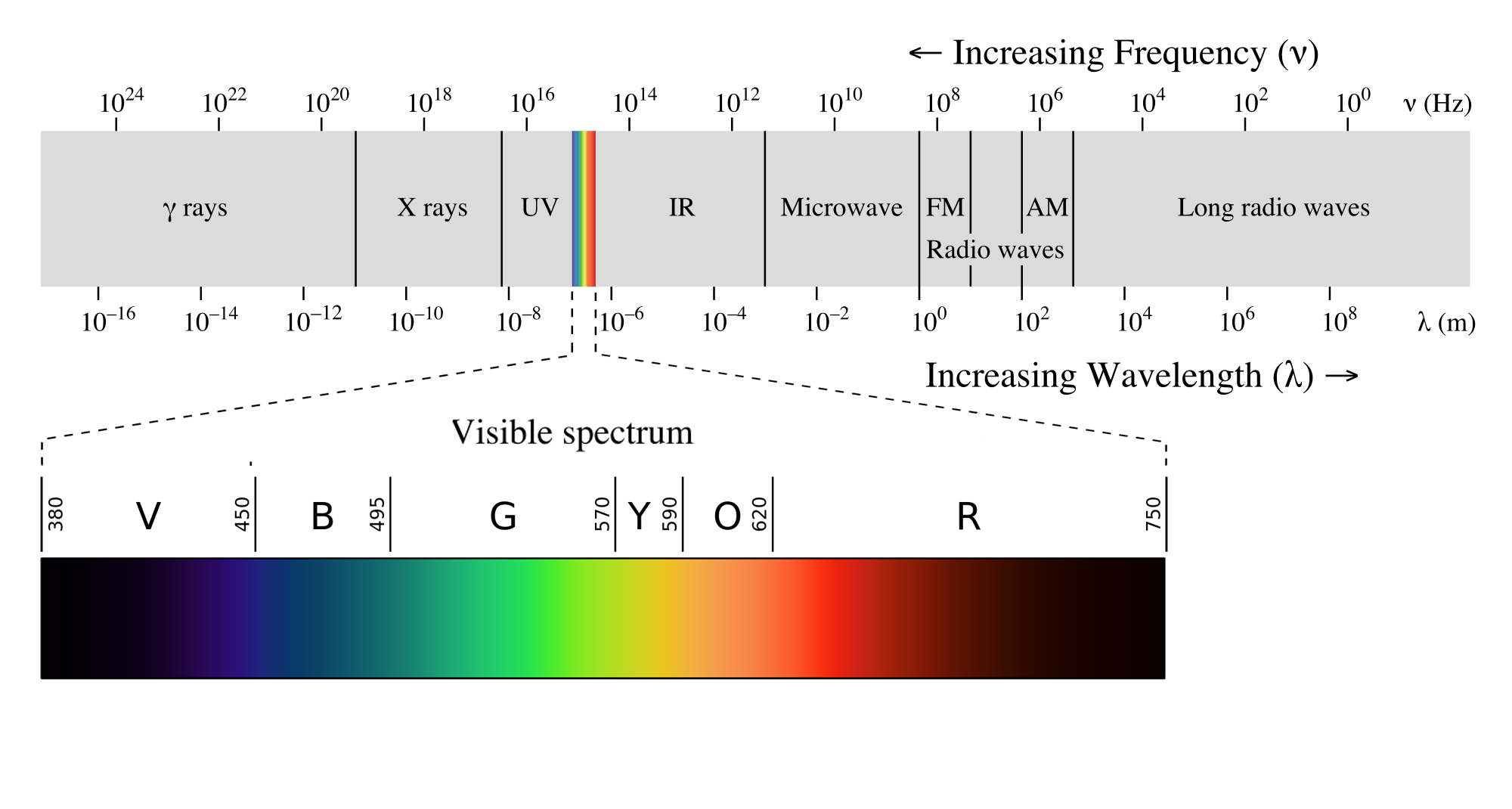
The whole electromagnetic spectrum, with a focus on visible light.
One of the problem of medicine is to be able to properly diagnose a patient ailment. Contrary to a mechanic, a doctor can't just open a patient just for the sake of analysis as it entails a lot of risk. The discovery of the ability to take photos of the inside of a patient body using those newly discovered x-rays was a huge step in medical diagnostic. Now you could properly observe a fracture or see the evolution of a lung disease. Medical imaging became a very important field of medicine and throughout the years have seen tremendous amount of innovation. Today, the 2 dimensional nature of the early radiography have been complemented by a third dimension either of time or space or even a fourth for multi-phase computed tomography images. X-rays can be generated in real-time in order to help doctor operate a patient without even opening him.
Indeed, one of the problem of x-rays is that they are dangerous. Due to their high energy level, they can ionize particles and modify the chemical properties of atoms. As a consequence they can break down DNA or, even worst, kill cells, which leads to pretty nasty consequences when their emissions are not properly controlled. Each time a doctor requests a CT exam, he is taking a risk. He has to weight the benefit of exposing his patient to dangerous ionizing rays versus the risk of not knowing exactly what is wrong with him. But fret not! X-rays are not the only mean to this end. Other type of medical imaging exists that are not inherently dangerous like Magnetic Resonance and Ultrasound.
Ultrasound of a human heart.
The combination of technology and outcome is called a modality. A CT scanner is a modality different from an MR scanner which itself is different from a US probe. And all these modalities will be used to diagnose different types of problems. The machine making up those modalities generate images that will then be used by doctors to diagnose and choose the best possible treatment. But how does those images get from the machine to the doctors eyes? Initially, radiography would be imprinted on a photographic film and would be reviewed directly by doctors. Storage was physical and the only way to see the image was to having it carried around physically. Various form of physical media were used up to a point were scanners and probes started to emit digital data. At that point, those images could finally be transmitted logically, copied, stored at different places and more importantly reviewed on a screen where image manipulation could enhance their diagnostic value. The screen on which doctors could see those images belongs to specific workstation purposefully build to review the medical images being generated.
There was one problem though. Multiple manufacturers competed on the medical imaging markets (mainly General Electric, Siemens, Philips and Toshiba) and none of them would produce medical images in the same way. As a consequence an image from a Toshiba scanner could not be read by a Siemens machine. In 1982, The American College of Radiology (ARC) and the National Electrical Manufacturers Association got together and decided to "specify a hardware interface, a minimum set of software commands, and a consistent set of data formats" which would allow interoperability between systems and a few years later in 1993, the ARC-NEMA standard was renamed Digital Imaging and Communications in Medicine (DICOM).
In the later parts of this series we will talk about the DICOM format in more detail and the way images are to be stored and processed in order to be useful (part 2) and we will dive into the nitty-gritty of how the information should be interpreted so that images come alive (part 3) and finally we will write a small algorithm which will allow us to render a Multiplanar Reformation (MPR) image. Stay tuned !
An historical CT scanner.
Next the DICOM format.